
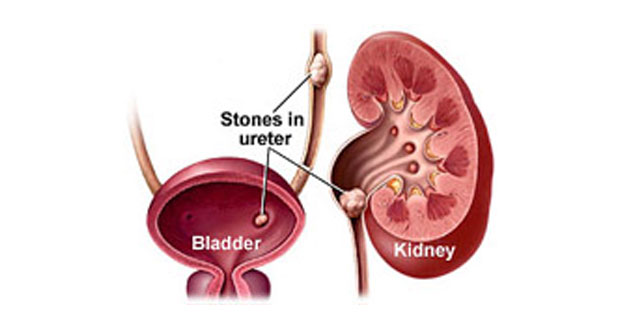
Kidney stones (calculi) are hardened mineral deposits that form in the kidney.
The kidneys filter waste products from the blood and add them to the urine that the kidneys produce. When waste materials in the urine do not dissolve completely, crystals and kidney stones are likely to form. These stones may stay in the kidney for a long time or they may pass out of the kidney and become lodged in the tube that carries urine from the kidney to the bladder (ureter). If left untreated, the kidney may swell and lose its function.
Stone Formation
Kidney stones form
- when there is a high level of calcium (hypercalciuria), oxalate (hyperoxaluria), or uric acid (hyperuricosuria) in the urine
- a lack of citrate in the urine,
- or insufficient water in the kidneys to dissolve waste products.
Signs and Symptoms
Stones that lodge in the tube that carries urine from the kidneys to the bladder (ureter) results in severe pain that begins in the loin and lower back and radiates to the groin or front of the lower abdomen.
A ‘small’ stone (usually 4 mm in diameter or less) has a 90% chance of spontaneous passage. Stones larger than 6 mm in diameter has less than 10% chance of passage.
Other symptoms of kidney stones may include the following:
- Blood in the urine (hematuria)
- Increased frequency of urination
- Nausea and vomiting
- Pain during urination (stinging, burning)
- Tenderness in the abdomen and kidney region
- Urinary tract infection (fever, chills, loss of appetite)
Diagnosis
Diagnosis of renal stone disease involves
- medical history,
- physical examination,
- laboratory evaluation,
- and imaging tests.
Imaging tests
Imaging tests used to diagnose kidney stones include:
- Ultrasound
Ultrasound can detect a dilated (swollen)) upper urinary tract and kidney caused by a stone lodged in the ureter, but usually cannot detect small stones, especially those located outside the kidney (in the ureter). It is the preferred imaging method for kidney stone patients who are pregnant.
- Intravenous Pyelogram (IVP)
This test involves taking a series of x-rays after injecting a contrast agent (dye) into a vein. Most kidney stones can be precisely located using this procedure. There is a slight risk for an allergic reaction to the contrast agent during this procedure and overall kidney function must be normal.
- Retrograde Pyelogram
This procedure eliminates the risk for an allergic reaction to the contrast agent because the dye does not reach the bloodstream, but it may require anesthesia. While retrograde pyelogram is the most reliable method for visualizing the urinary system and detecting stones, it is generally used only when other imaging methods are inadequate or unsuccessful.
- Computerized tomography (CT Scan)
This test uses a scanner and a computer to create images of the urinary system. It is performed quickly. CT scan can also help identify medical conditions (e.g., ruptured appendix, bowel obstruction) that cause symptoms similar to kidney stones. The non-contrast CT scan is the most common imaging test used to evaluate a possible kidney stones.
Treatment
- Treating kidney stone disease depends largely on the size, position and number of stones in urinary system.
- The majority of small stones (5 mm in diameter) that are not causing infection, blockage or symptoms will pass with an increased fluid intake.
- Pain that occurs when small stones start down the ureter can usually be treated with rest and analgesia.
- Certain types of stones, such as those made of uric acid, can be treated with medical therapy but majority of the stones are composed of calcium and are not responsive to medicine.
Indications for surgical intervention include
- Presence of infection
- Presence of obstruction
- Persistent colic with no advancement of the stone
- A stone more than 0.5 cm in diameter
Extracorporeal shock wave lithotripsy (ESWL)
 Extracorporeal Shock wave lithotripsy uses shock waves to break stone smaller than 2 cm into small fragments that can more easily flushed out of the urinary tract and pass out from the body. After identification of the position of the stone with X-ray or ultrasound, shockwaves are applied to fragment the stones. ESWL treatment can be used to treat urinary stones in the kidney and ureter (urine pipe that brings urine from kidney to bladder).
Extracorporeal Shock wave lithotripsy uses shock waves to break stone smaller than 2 cm into small fragments that can more easily flushed out of the urinary tract and pass out from the body. After identification of the position of the stone with X-ray or ultrasound, shockwaves are applied to fragment the stones. ESWL treatment can be used to treat urinary stones in the kidney and ureter (urine pipe that brings urine from kidney to bladder).
This procedure takes about 45 minute’s to1 hour, and is often done as an Outpatient Procedure. Intravenous analgesia is given to ensure a pain free experience. This procedure is very safe and causes no significant damage to the kidney. It can be repeated and may have to be repeated for larger or harder stones. Main drawback of the procedure is some stone are not well seen and some are hard to break.
Surgical intervention
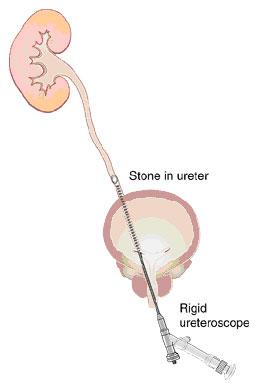
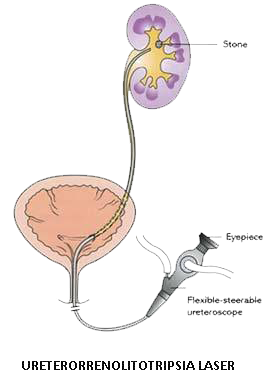
- Ureteroscopy – Involves the use of a scope that can be inserted up the urethra, through the bladder and into the ureter without an incision. Stones are fragmented using Holmium laser at Apollo Hospitals, chennai.Laser is universal energy source that breaks all stones. Laser breaks stones into powder and it has an added advantage that the fragment need not be removed from the ureter .There is no pain in the postoperative period as there is no fragments to pass as in case of standard lithoclast used for stone fragmentation.
- Open Surgery – Ureterolithotomy refers to the open surgical removal of a stone from the ureter.

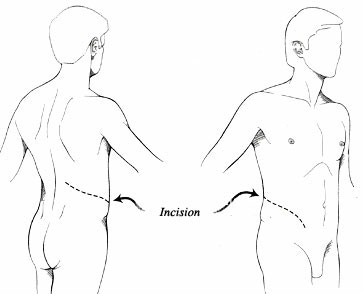
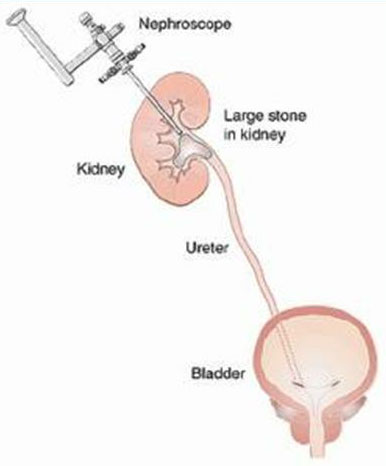
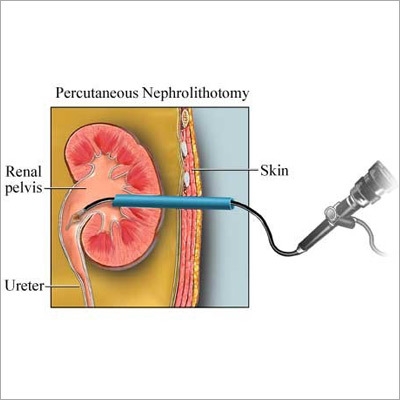
- Percutaneous surgery (PCNL) – Under anaesthesia a nephroscope is passed through an incision made in the flank area to locate and remove the stone. For larger stones, an ultrasonic probe may be needed to break the stone into small pieces.
- ESWL (Extracorporeal shock wave lithotripsy) – In ESWL, shock waves that are created outside the body travel through the skin and body tissues until they hit the stones. The stones break down into sand-like particles that are easily passed out through the urine.
- Repeat ESWL sessions may be necessary.
Laser
- Breaks any stones
- Less chances of leaving any fragments or residual stones
- Less complications
MINI PCNL
- Small incision compared to normal PCNL
- Less bleeding
- Less complications
- No stents
- No tubes

RIRS
- Small renal stones
- No incisions
- No risk of bleeding
- Patients whom PCNL is contra-indicated
Staghorn Calculi (Large stones, more than 2cm)
- Most staghorn stones are infection related and composed of calcium phosphate that results from infection with urease producing urinary pathogens.
- Staghorn stones lead to progressive obstruction, infection, and loss of kidney function therefore intervention is required
Staghorn Calculi – Treatment
Combinations of percutaneous stone removal and extracorporeal shock-wave lithotripsy (ESWL) are used remove staghorn calculi
How can I avoid getting more kidney stones?
- The most important thing you can do to prevent further stones forming is to drink lots of fluid.
- Drink at least three litres of fluid each day.
- Drink throughout the day and night if possible.
- While the best fluid is water, other suitable fluids are flavoured water and non-cola soft drinks (e.g. lemonade).
- You will know if you are drinking enough by the colour of your urine, which should be pale yellow to clear.
- Take the juice of one to two lemons (approximately 100mls daily). This can be diluted with water to drink over the course of the day.
- Reduce salt (sodium) intake: Keep salt in cooking to a minimum and do not add salt to meals. Avoid salty foods as much as possible such as:
- Marmite
- salted chips and nuts
- tinned and packet soups
- tinned meats,corned beef and smoked fish
- Moderate your protein intake: A high protein diet can increase calcium and oxalate excretion and this increases stone formation. Choose small to moderate serves of meat, fish, chicken, eggs, milk and dairy food.
- Adequate calcium intake: Surprisingly, a calcium restriction can encourage stone formation. As such, you should aim to have the recommended daily allowance for calcium. For adults the recommended daily allowance is approximately 800 milligrams which can be achieved by choosing three to four small to moderate servings of milk and dairy foods (e.g. one serve = a pottle of yoghurt, a glass of milk) per day.
- Other restrictions: You will be informed by your health professional if further dietary restrictions such as limiting oxalate-containing foods are required.
- Caution: If you are taking any herbal, vitamin or dietary supplements or antacids, please check with your health professional as these may increase your risk of forming stones.